
Towards Standardisation of Technique for En Bloc Sacrectomy for Locally Advanced and Recurrent Rectal Cancer

 and
and
Abstract
:1. Introduction
2. Preoperative Evaluation
3. Operative Steps
3.1. Patient Preparation and Position
3.2. Visceral Mobilisation
3.3. Vascular Mobilisation and Control
3.4. Nerve Root Identification
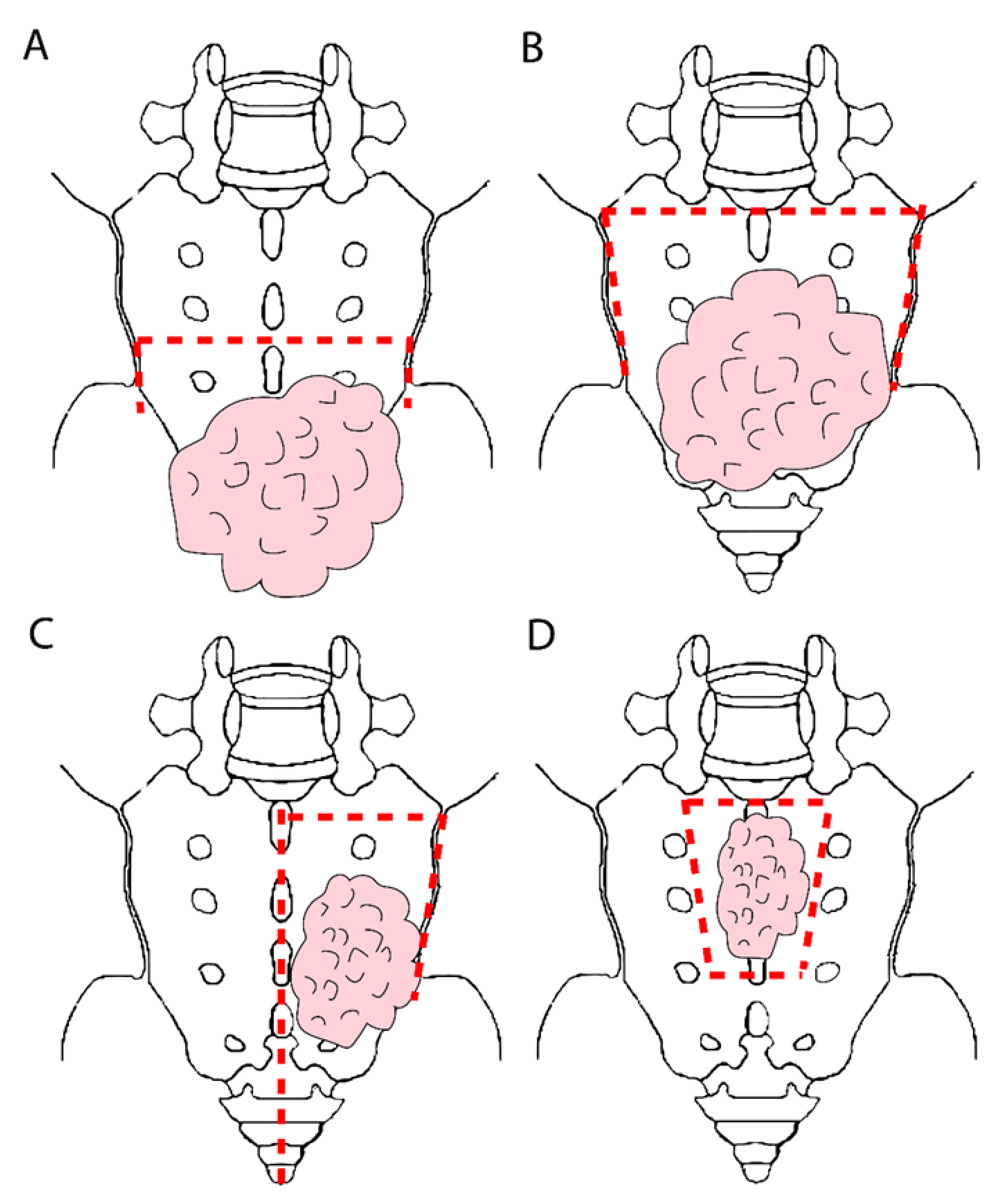
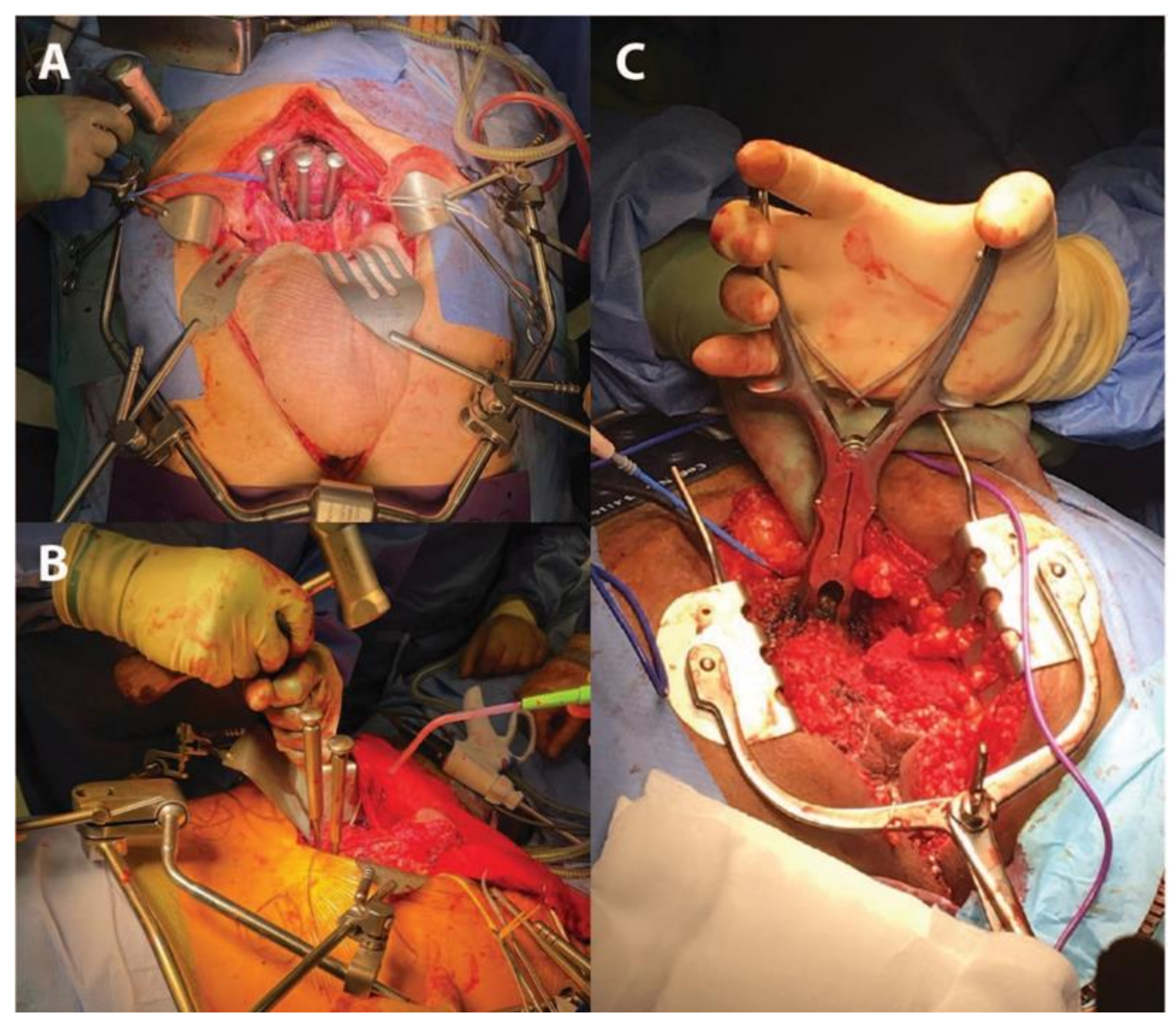
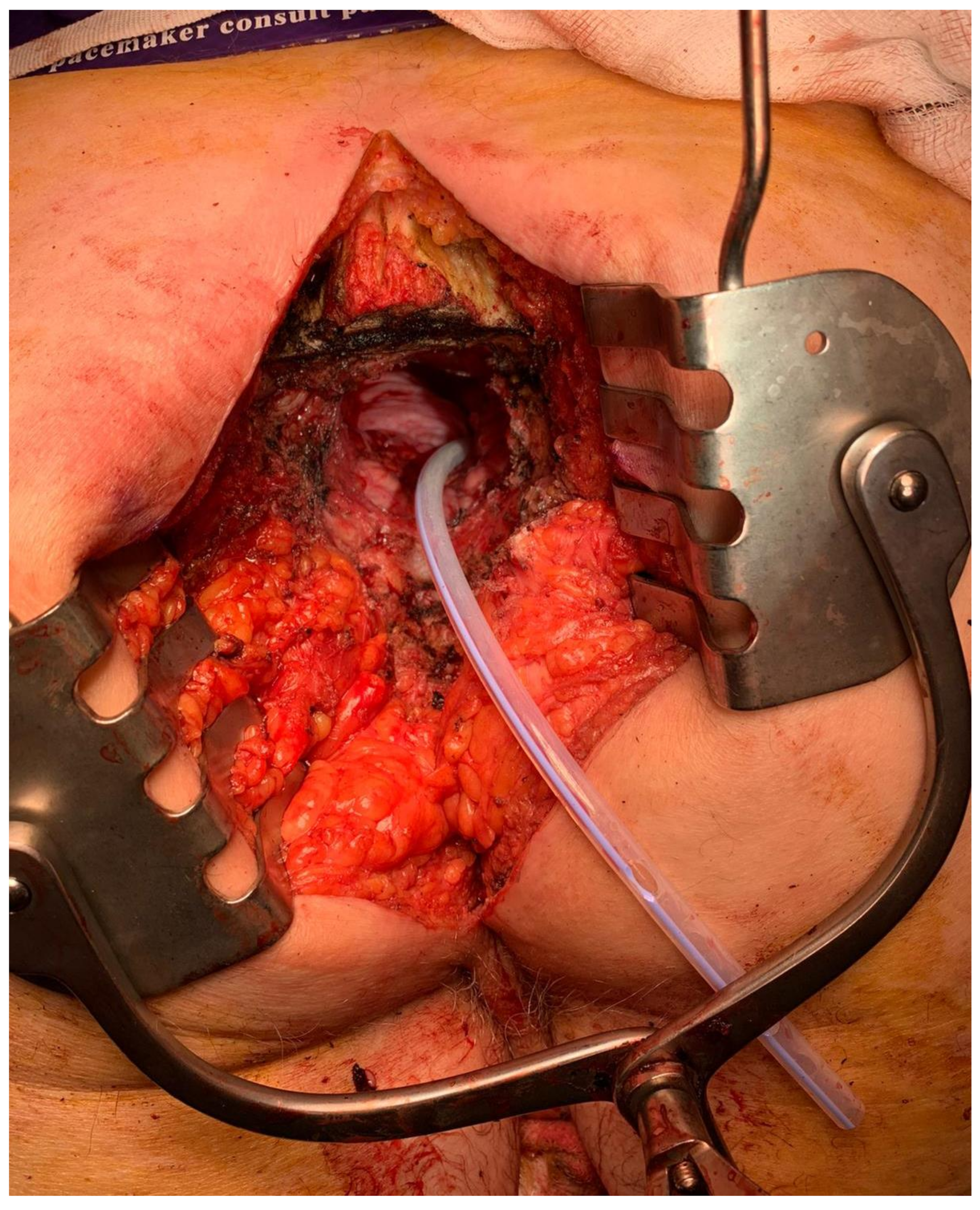
3.5. Sacral Division and Specimen Extraction
3.6. Reconstruction Options
3.7. Special Cases-Modified Partial Sacrectomy
3.8. Minimially Invasive En Bloc Sacrectomy
4. Postoperative Complications
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cheung, F.; Sandhu, J.S. Voiding dysfunction after non-urologic pelvic surgery. Curr. Urol. Rep. 2018, 19, 75. [Google Scholar] [CrossRef]
- Sasikumar, A.; Bhan, C.; Jenkins, J.T.; Antoniou, A.; Murphy, J. Systematic review of pelvic exenteration with en bloc sacrectomy for recurrent rectal adenocarcinoma: R0 resection predicts disease-free survival. Dis. Colon Rectum 2017, 60, 346–352. [Google Scholar] [CrossRef]
- McCarthy, A.S.; Solomon, M.J.; Koh, C.E.; Firouzbakht, A.; Jackson, S.A.; Steffens, D. Quality of life and functional outcomes following pelvic exenteration and sacrectomy. Color. Dis. 2020, 22, 521–528. [Google Scholar] [CrossRef]
- Bhangu, A.; Brown, G.; Akmal, M.; Tekkis, P. Outcome of abdominosacral resection for locally advanced primary and recurrent rectal cancer. Br. J. Surg. 2012, 99, 1453–1461. [Google Scholar] [CrossRef]
- Bonello, V.A.; Bhangu, A.; Fitzgerald, J.E.F.; Rasheed, S.; Tekkis, P. Intraoperative bleeding and haemostasis during pelvic surgery for locally advanced or recurrent rectal cancer: A prospective evaluation. Tech. Coloproctol. 2014, 18, 887–893. [Google Scholar] [CrossRef]
- Kido, A.; Koizumi, M.; Honoki, K.; Tanaka, Y.; Koyama, F.; Nakajima, Y.; Akahane, M. Extent and contraindications for sacral amputation in patients with recurrent rectal cancer: A systematic literature review. J. Orthop. Sci. 2011, 16, 286–290. [Google Scholar] [CrossRef]
- Koh, C.E.; Solomon, M.; Brown, K.G.; Austin, K.; Byrne, C.M.; Lee, P.; Young, J.M. The evolution of pelvic exenteration practice at a single center: Lessons learned from over 500 cases. Dis. Colon Rectum 2017, 60, 627–635. [Google Scholar] [CrossRef]
- Shaikh, I.; Holloway, I.; Aston, W.; Littler, S.; Burling, D.; Antoniou, A.; Jenkins, J.T.; Complex Cancer Clinic St. Mark’s Hospital London. High subcortical sacrectomy: A novel approach to facilitate complete resection of locally advanced and recurrent rectal cancer with high (S1–S2) sacral extension. Color. Dis. 2015, 18, 386–392. [Google Scholar] [CrossRef]
- Dozois, E.; Privitera, A.; Holubar, S.; Aldrete, J.; Sim, F.; Rose, P.; Walsh, M.; Bower, T.; Leibovich, B.; Nelson, H.; et al. High sacrectomy for locally recurrent rectal cancer: Can long-term survival be achieved? J. Surg. Oncol. 2011, 103, 105–109. [Google Scholar] [CrossRef]
- Melich, G.; Weber, M.; Stein, B.; Minutolo, V.; Arena, M.; Arena, G.O. Total sacrectomy for recurrent rectal cancer—A case report featuring technical details and potential pitfalls. Int. J. Surg. Case Rep. 2014, 5, 403–407. [Google Scholar] [CrossRef] [Green Version]
- Solomon, M.J.; Tan, K.-K.; Bromilow, R.G.; Al-Mozany, N.; Lee, P.J. Sacrectomy via the abdominal approach during pelvic exenteration. Dis. Colon Rectum 2014, 57, 272–277. [Google Scholar] [CrossRef]
- Temple, W.J.; Ketcham, A.S. Sacral resection for control of pelvic tumors. Am. J. Surg. 1992, 163, 370–374. [Google Scholar] [CrossRef]
- Lau, Y.C.; Brown, K.G.M.; Lee, P. Pelvic exenteration for locally advanced and recurrent rectal cancer—How much more? J. Gastrointest. Oncol. 2019, 10, 1207–1214. [Google Scholar] [CrossRef]
- Lee, D.J.-K.; Sagar, P.M.; Sadadcharam, G.; Tan, K.-Y. Advances in surgical management for locally recurrent rectal cancer: How far have we come? World J. Gastroenterol. 2017, 23, 4170–4180. [Google Scholar] [CrossRef] [PubMed]
- Kanjanasilp, P.; Ng, J.L.; Kajohnwongsatit, K.; Thiptanakit, C.; Limvorapitak, T.; Sahakitrungruang, C. Anatomical variations of iliac vein tributaries and their clinical implications during complex pelvic surgeries. Dis. Colon Rectum 2019, 62, 809–814. [Google Scholar] [CrossRef]
- Coker, D.J.; Austin, K.K.S.; Eyers, A.A.; Young, C.J. Pre-emptive triple tributary internal iliac vein ligation reduces catastrophic haemorrhage from sacrectomy during pelvic exenterative surgery. Tech. Coloproctol. 2017, 21, 445–450. [Google Scholar] [CrossRef]
- Moriya, Y.; Akasu, T.; Fujita, S.; Yamamoto, S. Total pelvic exenteration with distal sacrectomy for fixed recurrent rectal cancer in the pelvis. Dis. Colon Rectum 2004, 47, 2047–2054. [Google Scholar] [CrossRef] [PubMed]
- Milne, T.; Solomon, M.J.; Lee, P.; Young, J.M.; Stalley, P.; Harrison, J.D. Assessing the impact of a sacral resection on morbidity and survival after extended radical surgery for locally recurrent rectal cancer. Ann. Surg. 2013, 258, 1007–1013. [Google Scholar] [CrossRef]
- Khaled, F.; Smith, M.J.; Moises, C.; Smith, A.J.; Yee, A.J.M. Single-stage anterior high sacrectomy for locally recurrent rectal cancer. Spine 2014, 39, 443–452. [Google Scholar] [CrossRef]
- Crowe, P.J.; Temple, W.J.; Lopez, M.J.; Ketcham, A.S. Pelvic exenteration for advanced pelvic malignancy. Semin. Surg. Oncol. 1999, 17, 152–160. [Google Scholar] [CrossRef]
- Roldan, H.; Perez-Orribo, L.F.; Plata-Bello, J.M.; Martin-Malagon, A.I.; Garcia-Marin, V.M. Anterior-only partial sacrectomy for en bloc resection of locally advanced rectal cancer. Glob. Spine J. 2014, 4, 273–277. [Google Scholar] [CrossRef] [Green Version]
- Aydin, C.; Kayaalp, C.; Cetin, A. Sacrectomy margins for rectal cancer invading sacrum: An anatomic study. J. Surg. Oncol. 2011, 103, 742–743. [Google Scholar] [CrossRef]
- Pareekutty, N.M.; Balasubramanian, S.; Kadam, S.; Jayaprakash, D.; Ankalkoti, B.; Nayanar, S.; Muttath, G.; Anilkumar, B. En bloc resection with partial sacrectomy helps to achieve R0 resection in locally advanced rectal cancer, experience from a tertiary cancer center. Indian J. Surg. Oncol. 2019, 10, 141–148. [Google Scholar] [CrossRef]
- Lee, D.J.K.; Wang, K.Y.; Sagar, P.M.; Timothy, J. S1 Sacrectomy for re-recurrent rectal cancer: Our experience with reconstruction using an expandable vertebral body replacement device. Dis. Colon Rectum 2018, 61, 261–265. [Google Scholar] [CrossRef]
- Magrini, S.; Nelson, H.; Gunderson, L.L.; Sim, F.H. Sacropelvic resection and intraoperative electron irradiation in the management of recurrent anorectal cancer. Dis. Colon Rectum 1996, 39, 1–9. [Google Scholar] [CrossRef]
- Meltonmeaux, G.B.; Paty, P.B.; Boland, P.J.; Healey, J.; Savatta, S.G.; Casas-Ganem, J.E.; Guillem, J.G.; Weiser, M.R.; Cohen, A.M.; Minsky, B.D.; et al. Sacral resection for recurrent rectal cancer: Analysis of morbidity and treatment results. Dis. Colon Rectum 2006, 49, 1099–1107. [Google Scholar] [CrossRef]
- Williams, C.P.; Reynolds, H.L.; Delaney, C.P.; Champagne, B.; Obias, V.; Joh, Y.-G.; Merlino, J.; Kinsella, T.J. Clinical results of intraoperative radiation therapy for patients with locally recurrent and advanced tumors having colorectal involvement. Am. J. Surg. 2008, 195, 405–409. [Google Scholar] [CrossRef]
- Glimelius, B. Recurrent rectal cancer. The pre-irradiated primary tumour: Can more radiotherapy be given? Colorectal Dis. 2003, 5, 501–503. [Google Scholar] [CrossRef]
- Guo, S.; Reddy, C.A.; Kolar, M.; Woody, N.; Mahadevan, A.; Deibel, F.C.; Dietz, D.W.; Remzi, F.H.; Suh, J.H. Intraoperative radiation therapy with the photon radiosurgery system in locally advanced and recurrent rectal cancer: Retrospective review of the Cleveland clinic experience. Radiat. Oncol. 2012, 7, 110. [Google Scholar] [CrossRef] [Green Version]
- Boyle, K.M.; Sagar, P.M.; Chalmers, A.G.; Sebag-Montefiore, D.; Cairns, A.; Eardley, I. Surgery for locally recurrent rectal cancer. Dis. Colon Rectum 2005, 48, 929–937. [Google Scholar] [CrossRef]
- Di Mauro, D.; D’Hoore, A.; Penninckx, F.; De Wever, I.; Vergote, I.; Hierner, R.V.-Y. Bilateral gluteus maximus myocutaneous advancement flap in the reconstruction of large perineal defects after resection of pelvic malignancies. Colorectal Dis. 2009, 11, 508–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diaz, J.; McDonald, W.S.; Armstrong, M.; Eismont, F.; Hellinger, M.; Thaller, S. Reconstruction after extirpation of sacral malignancies. Ann. Plast. Surg. 2003, 51, 126–129. [Google Scholar] [CrossRef]
- Grinsell, D.G.; Morrison, E.; Tansley, P.D.T. The inferior gluteal artery myocutaneous flap with vascularized fascia lata to reconstruct extended abdominoperineal defects. Plast. Reconstr. Surg. 2013, 132, 836e–840e. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.G.M.; Solomon, M.J.; Austin, K.K.S.; Lee, P.J.; Stalley, P. Posterior high sacral segmental disconnection prior to anterior en bloc exenteration for recurrent rectal cancer. Tech. Coloproctol. 2016, 20, 401–404. [Google Scholar] [CrossRef]
- Evans, M.; Harji, D.P.; Sagar, P.M.; Wilson, J.; Koshy, A.; Timothy, J.; Giannoudis, P.V. Partial anterior sacrectomy with nerve preservation to treat locally advanced rectal cancer. Color. Dis. 2013, 15, e336–e339. [Google Scholar] [CrossRef] [PubMed]
- Herd, A.J.; Solomon, M.J. The Advanced Primary or Recurrent Rectal Cancer: Pushing the Boundaries. Coloproctology: A Practical Guide; Beynon, J., Harris, D., Davies, M., Evans, M., Eds.; Springer: Berlin, Germany, 2017. [Google Scholar]
- Uemura, M.; Ikeda, M.; Kawai, K.; Nishimura, J.; Takemasa, I.; Mizushima, T.; Yamamoto, H.; Sekimoto, M.; Doki, Y.; Mori, M. Laparoscopic surgery using a Gigli wire saw for locally recurrent rectal cancer with concomitant intraperitoneal sacrectomy. Asian J. Endosc. Surg. 2018, 11, 83–86. [Google Scholar] [CrossRef] [Green Version]
- Rayhanabad, J.; Sassani, P.; Abbas, M.A. Laparoscopic repair of perineal hernia. JSLS 2009, 13, 237–241. [Google Scholar]
- Manrique, O.J.; Rajesh, A.; Asaad, M.; Bakri, K.; Tran, N.V.; Houdek, M.T.; Dozois, E.J.; Rose, P.S. Surgical outcomes after abdominoperineal resection with sacrectomy and soft tissue reconstruction: Lessons learned. J. Reconstr. Microsurg. 2020, 36, 064–072. [Google Scholar] [CrossRef] [PubMed]
- Davidge, K.M.; Raghuram, K.; Hofer, S.O.P.; Ferguson, P.C.; Wunder, J.S.; Swallow, C.J.; Zhong, T. Impact of flap reconstruction on perineal wound complications following ablative surgery for advanced and recurrent rectal cancers. Ann. Surg. Oncol. 2014, 21, 2068–2073. [Google Scholar] [CrossRef]
- Harris, C.; Solomon, M.; Heriot, A.G.; Sagar, P.M.; Tekkis, P.P.; Dixon, L.; Pascoe, R.; Dobbs, B.R.; Frampton, C.M.; Harji, D.P.; et al. The outcomes and patterns of treatment failure after surgery for locally recurrent rectal cancer. Ann. Surg. 2016, 264, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.S.-Y.; Koh, C.E.; Liu, H.; Solomon, M.J.; Johnstone, C.S. The price we pay for radical curative pelvic exenterations: Prevalence and management of pain. Dis. Colon Rectum 2018, 61, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Davidge, K.; Eskicioglu, C.; Lipa, J.; Ferguson, P.; Swallow, C.; Wright, F. Qualitative assessment of patient experiences following sacrectomy. J. Surg. Oncol. 2010, 101, 447–450. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| En Bloc Sacrectomy for Rectal Cancer—Operative Steps | |
|---|---|
| Patient preparation and position | High sacrectomy: mixed supine/prone approach required Low sacrectomy: mixed supine/prone approach or totally supine approach feasible |
| Visceral mobilisation | Start with anterolateral pelvic structures first Clear midline of anterior sacrum to predetermined transection point |
| Vascular mobilisation and control | Ureterolysis and external iliac mobilisation External iliac artery control Dissect free the medial psoas borders Identify L5 and control internal iliac artery Selective internal iliac branch ligation |
| Nerve root identification | Identify sciatic nerve roots exiting their foramina below L5 Transect branches below planned sacral division |
| Sacral division and specimen extraction | Extend clearance of anterior sacral cortex laterally to planned transection line Diathermy mark transection level Osteotome x 3 through premarked point, starting midline and then bilaterally Alternatively use pneumatic drill or Gigli saw Divide posterior sacral soft tissue attachments and remove via perineal or prone approach Haemostasis |
| Reconstruction | Visceral restoration of continuity/ostomy +/− omental flap/mesh for pelvic defect +/− bony reconstruction Myofasciocutaneous flaps, most commonly now raised on the superior gluteal arteries |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rogers, A.C.; Jenkins, J.T.; Rasheed, S.; Malietzis, G.; Burns, E.M.; Kontovounisios, C.; Tekkis, P.P. Towards Standardisation of Technique for En Bloc Sacrectomy for Locally Advanced and Recurrent Rectal Cancer. J. Clin. Med. 2021, 10, 4921. https://doi.org/10.3390/jcm10214921
Rogers AC, Jenkins JT, Rasheed S, Malietzis G, Burns EM, Kontovounisios C, Tekkis PP. Towards Standardisation of Technique for En Bloc Sacrectomy for Locally Advanced and Recurrent Rectal Cancer. Journal of Clinical Medicine. 2021; 10(21):4921. https://doi.org/10.3390/jcm10214921
Chicago/Turabian StyleRogers, Ailín C., John T. Jenkins, Shahnawaz Rasheed, George Malietzis, Elaine M. Burns, Christos Kontovounisios, and Paris P. Tekkis. 2021. "Towards Standardisation of Technique for En Bloc Sacrectomy for Locally Advanced and Recurrent Rectal Cancer" Journal of Clinical Medicine 10, no. 21: 4921. https://doi.org/10.3390/jcm10214921