
Oral Chagas Disease in Colombia—Confirmed and Suspected Routes of Transmission

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Clinical Manifestations of Oral Chagas Disease
3. Oral T. cruzi Transmission Pathogenicity
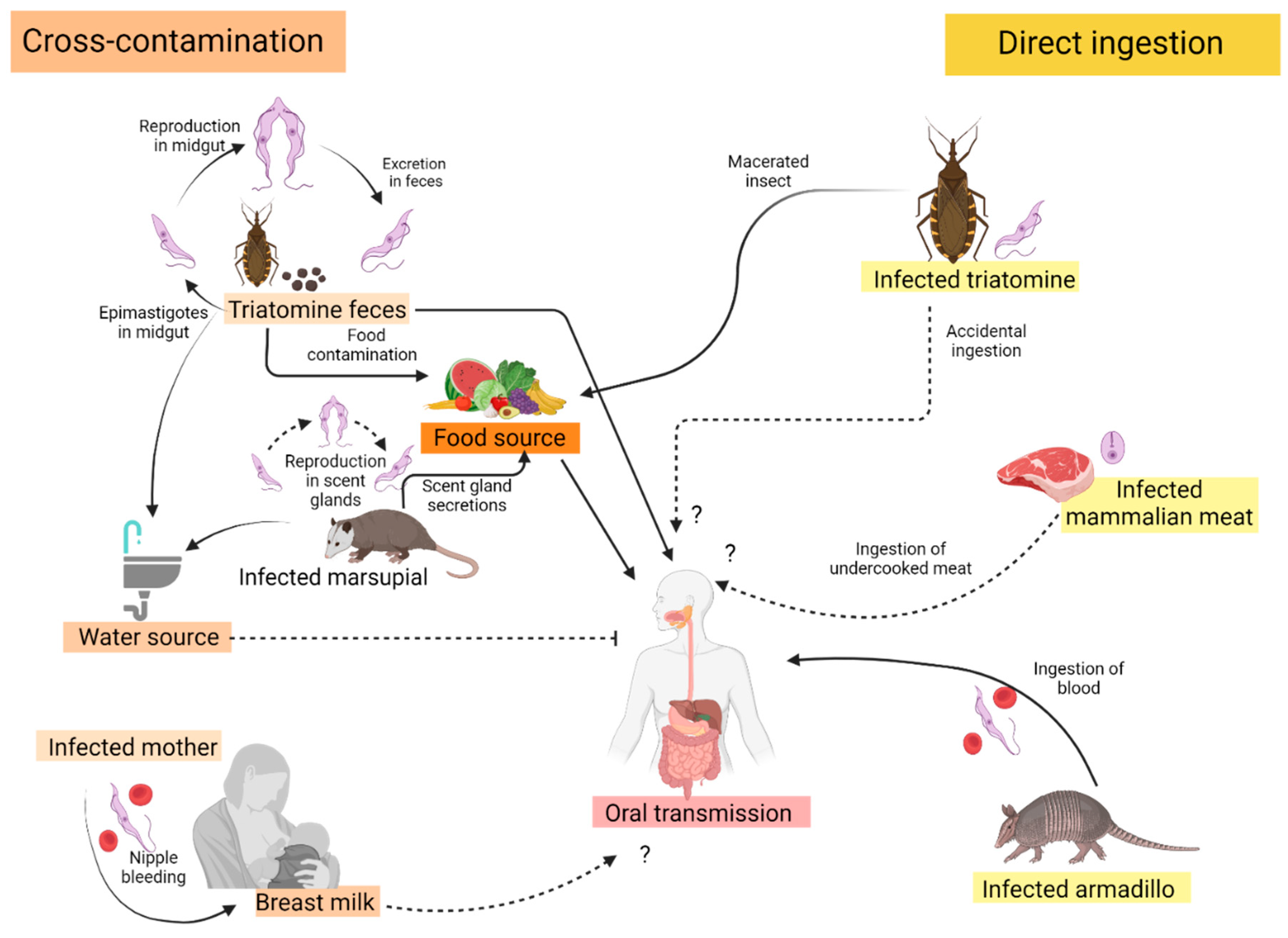
4. T. cruzi Contaminated Food and Drink
4.1. Ingestion of T. cruzi Contaminated Fruit Juices and Foods
4.2. Consumption of T. cruzi Infected Mammalian Meat
4.3. Ingestion of Infected Mammalian Blood
4.4. Other Unique Forms of T. cruzi Oral Ingestion
5. Peridomestic Triatomines Associated with Oral T. cruzi Transmission
6. Opossums and Odoriferous Gland T. cruzi-Infected Secretions
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pérez-Molina, J.A.; Molina, I. Chagas disease. Lancet 2018, 391, 82–94. [Google Scholar] [CrossRef] [PubMed]
- Coura, J.R. The main sceneries of Chagas disease transmission. The vectors, blood and oral transmissions—A comprehensive review. Mem. Inst. Oswaldo Cruz 2015, 110, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Velásquez-Ortiz, N.; Ramírez, J.D. Understanding the oral transmission of Trypanosoma cruzi as a veterinary and medical foodborne zoonosis. Res Vet. Sci. 2020, 132, 448–461. [Google Scholar] [CrossRef] [PubMed]
- Franco-Paredes, C.; Villamil-Gómez, W.E.; Schultz, J.; Henao-Martínez, A.F.; Parra-Henao, G.; Rassi, A.J.R. A deadly feast: Elucidating the burden of orally acquired acute Chagas disease in Latin America-Public health and travel medicine importance. Travel Med. Infect. Dis. 2020, 36, 101565. [Google Scholar] [CrossRef]
- Cantillo-Barraza, O.; Torres, J.; Hernández, C.; Romero, Y.; Zuluaga, S.; Correa-Cárdenas, C.A. The potential risk of enzootic Trypanosoma cruzi transmission inside four training and re-training military battalions (BITER) in Colombia. Parasite Vectors 2021, 14, 519. [Google Scholar] [CrossRef]
- Parra-Henao, G.; Oliveros, H.; Hotez, P.J.; Motoa, G.; Franco-Paredes, C.; Henao-Martínez, A.F. In Search of Congenital Chagas Disease in the Sierra Nevada de Santa Marta, Colombia. Am. J. Trop. Med. Hyg. 2019, 101, 482–483. [Google Scholar] [CrossRef]
- Cucunubá, Z.M.; Nouvellet, P.; Conteh, L.; Vera, M.J.; Angulo, V.M.; Dib, J.C. Modelling historical changes in the force-of-infection of Chagas disease to inform control and elimination programmes: Application in Colombia. BMJ Glob. Health 2017, 2, e000345. [Google Scholar] [CrossRef]
- Guhl, F. Chagas disease in Andean countries. Mem. Inst. Oswaldo Cruz 2007, 102 (Suppl. 1), 29–38. [Google Scholar] [CrossRef]
- Zuluaga, S.; Mejía, P.; Vélez-Mira, A.; Quintero, J.; Triana-Chávez, O.; Cantillo-Barraza, O. Updated geographical distribution and natural infection of Panstrongylus geniculatus (Latreille, 1811) in Antioquia department, Colombia. Parasite Epidemiol. Control. 2021, 15, e00226. [Google Scholar] [CrossRef]
- Cantillo-Barraza, O.; Medina, M.; Zuluaga, S.; Blanco, M.I.; Caro, R.; Jaimes-Dueñez, J. Distribution and natural infection status of synantrophic triatomines (Hemiptera: Reduviidae), vectors of Trypanosoma cruzi, reveals new epidemiological scenarios for chagas disease in the Highlands of Colombia. PLoS Negl. Trop. Dis. 2021, 15, e0009574. [Google Scholar] [CrossRef]
- da Silva, N.N.; Clausell, D.T.; Nólibos, H.; de Mello, A.L.; Ossanai, J.; Rapone, T.; Snell, T. Surto epidêmico de doença de Chagas com provavel contaminação oral [Epidemic outbreak of Chagas disease probably due to oral contamination]. Rev. Inst. Med. Trop. Sao Paulo 1968, 10, 265–276. [Google Scholar] [PubMed]
- Nery-Guimarães, F.; Silva, N.; Clausell, D.T.; Mello, A.L.; Rapone, T.; Snell, T. Um surto epidêmico de doença de Chagas de provável transmissão digestiva, ocorrido em Teutônia (Estrela, Rio Grande do Sul). Hospital 1968, 73, 1767–1804. [Google Scholar]
- de Noya, B.A.; Dias-Bello, Z.; Colmenares, C.; Ruiz-Guevara, R.; Mauriello, L.; Zavala-Jaspe, R.; Suarez, J.A.; Abate, T.; Naranjo, L.; Paiva, M.; et al. Large urban outbreak of orally acquired acute Chagas disease at a school in Caracas, Venezuela. J. Infect. Dis. 2010, 201, 1308–1315. [Google Scholar] [CrossRef] [PubMed]
- Hernández, C.; Vera, M.J.; Cucunubá, Z.; Flórez, C.; Cantillo, O.; Buitrago, L.S. High-Resolution Molecular Typing of Trypanosoma cruzi in 2 Large Outbreaks of Acute Chagas Disease in Colombia. J. Infect. Dis. 2016, 214, 1252–1255. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, N. Molecular mechanisms of Trypanosoma cruzi infection by oral route. Mem. Inst. Oswaldo Cruz 2009, 104 (Suppl. S1), 101–107. [Google Scholar] [CrossRef]
- Maeda, F.Y.; Clemente, T.M.; Macedo, S.; Cortez, C.; Yoshida, N. Host cell invasion and oral infection by Trypanosoma cruzi strains of genetic groups TcI and TcIV from chagasic patients. Parasites Vectors 2016, 9, 189. [Google Scholar] [CrossRef]
- Gual-Gonzalez, L.; Arango-Ferreira, C.; Lopera-Restrepo, L.C.; Cantillo-Barraza, O.; Marín, D.V.; Bustamante, N.R. Acute Pediatric Chagas Disease in Antioquia, Colombia: A Geographic Location of Suspected Oral Transmission. Microorganisms 2021, 10, 8. [Google Scholar] [CrossRef]
- Rincón-Acevedo, C.Y.; Parada-García, A.S.; Olivera, M.J.; Torres-Torres, F.; Zuleta-Dueñas, L.P.; Hernández, C.; Ramírez, J.D. Clinical and Epidemiological Characterization of Acute Chagas Disease in Casanare, Eastern Colombia, 2012–2020. Front. Med. 2021, 8, 681635. [Google Scholar] [CrossRef]
- Bohórquez, R.M.B.; Blanco, M.; Nicholls, R.S.; Hernández, C.A.; Gualdrón, L. Estudio de una epidemia de carditis aguda en población adulta. Act. Med. Col. 1992, 17, 4. [Google Scholar]
- Cáceres, D.; Nicholls, R.S.; Corredor, A.; Gualdrón, L.; Slait, E.; Dib, J.; Ariza, K. Investigación de un brote de síndrome febril con miocarditis aguda en Guamal, Magdalena, 7 a 11 de junio de 1999. Inf. Quinc. Epidemiol. Nac. 1999, 4, 170–178. [Google Scholar]
- Hernández, L.M.; Ramírez, A.N.; Cucunuba, Z.M.; Zambrano, P. Brote de Chagas agudo en Lebrija, Santander 2008. Rev. Del. Obs. Salud Públca Santander. 2009, 1, 28–36. [Google Scholar]
- Zambrano, P.; Cucunubá, Z.M.; Montilla, M.; Flórez, A.; Parra, E.; Cortes, L. Brotes de síndrome febril asociado a miocarditis aguda chagásica de possible transmisión oral en el departamento de Santander, diciembre de 2008 a mayo de 2009. Inf. Quinc. Epidemiol. Nac. 2010, 15, 17–32. [Google Scholar]
- Ramírez, J.D.; Montilla, M.; Cucunubá, Z.M.; Floré, A.C.; Zambrano, P.; Guhl, F. Molecular Epidemiology of Human Oral Chagas Disease Outbreaks in Colombia. PLoS Negl. Trop. Dis. 2013, 7, e2041. [Google Scholar] [CrossRef] [PubMed]
- Rueda, K.; Trujillo, J.E.; Carranza, J.C.; Vallejo, G. Transmisión oral de Trypanosoma cruzi: Una nueva situación epidemio-lógica de la enfermedad de Chagas en Colombia y otros países suramericanos. Biomédica 2014, 34, 631–641. [Google Scholar] [CrossRef] [PubMed]
- Soto, H.; Tibaduiza, T.; Montilla, M.; Triana, O.; Suárez, D.C.; Torres, M.T.; Arias, M.T.; Lugo, L. Investigación de vec-tores y reservorios en brote de Chagas agudo por posible transmisión oral en Aguachica, Cesar, Colombia. Cad. Saúde Públca 2014, 30, 746–756. [Google Scholar] [CrossRef] [PubMed]
- Ríos, J.F.; Arboleda, M.; Montoya, A.N.; Alarcón, E.P. Probable outbreak of oral trans-mission of Chagas disease in Turbo, Antioquia. Biomédica 2011, 31, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Zuleta-Dueñas, L.P.; Lopez-Quiroga, A.J.; Torres-Torres, F.; Castañeda-Porras, O. Posible transmisión oral de la enferme-dad de Chagas en trabajadores del sector de los hidrocarburos en Casanare, Colombia, 2014. Rev. Biomed. 2017, 37, 2. [Google Scholar]
- Prensa Libre Casanare. 3 December 2015. Available online: https://prensalibrecasanare.com/salud/18663-investigan-casos-de-chagas-por-posible-transmisiun-oral-en-trinidad.html (accessed on 20 December 2023).
- Institudo National de Salud, Boletín Epidemiológico Semanal. 18 November 2017. Available online: https://www.ins.gov.co/buscador-eventos/BoletinEpidemiologico/2017%20Boletín%20epidemiológico%20semana%2018.pdf (accessed on 20 December 2023).
- Prensa Libre Casanare. 22 May 2017. Available online: https://prensalibrecasanare.com/salud/25205-una-familia-de-paz-de-ariporo-vnctima-de-brote-de-enfermedad-de-chagas-agudo.html (accessed on 20 December 2023).
- Institudo National de Salud, Boletín Epidemiológico Semanal. Semana Epidemiológico 33. 2019. Available online: https://www.ins.gov.co/buscadoreventos/BoletinEpidemiologico/2019%20Bolet%C3%ADn%20epidemiol%C3%B3gico%20semana%2033.pdf (accessed on 20 December 2023).
- Prensa Libre Casanare. 6 May 2020. Available online: https://prensalibrecasanare.com/salud/37356-brote-agudo-de-chagas-en-vereda-de-yopal.html (accessed on 20 December 2023).
- Institudo National de Salud, Boletín Epidemiológico Semanal. Semana Epidemiológico 20. 2021. Available online: https://www.ins.gov.co/buscador-eventos/BoletinEpidemiologico/2021_Boletin_epidemiologico_semana_50.pdf (accessed on 20 December 2023).
- Institudo National de Salud, Boletín Epidemiológico Semanal. Semana Epidemiológico 6. 2021. Available online: https://www.ins.gov.co/buscador-eventos/BoletinEpidemiologico/2021_Boletin_epidemiologico_semana_6.pdf (accessed on 20 December 2023).
- Gutiérrez, S.A.; Jaimes-Dueñez, J.; Cruz-Saavedra, L.; Hernández, C.; Cantillo-Barraza, O.; Álvarez, F.; Blanco, M.; Leal, B.; Martínez, L.; Medina, M.; et al. An Outbreak of Acute Chagas Disease Possibly Spread through Oral Transmission Involving Animal Reservoirs in Eastern Colombia. Am. J. Trop. Med. Hyg. 2023, tpmd230380, Advance online publication. [Google Scholar] [CrossRef]
- Institudo National de Salud, Boletín Epidemiológico Semanal. Semana Epidemiológico 11. 2022. Available online: https://www.ins.gov.co/buscador-eventos/BoletinEpidemiologico/2022_Boletín_epidemiologico_semana_11.pdf (accessed on 20 December 2023).
- Institudo National de Salud, Boletín Epidemiológico Semanal. Semana Epidemiológico 18. 2022. Available online: https://www.ins.gov.co/buscador-eventos/BoletinEpidemiologico/2022_Boletin_epidemiologico_semana_18.pdf (accessed on 20 December 2023).
- Institudo National de Salud, Boletín Epidemiológico Semanal. Semana Epidemiológico 14. 2023. Available online: https://www.ins.gov.co/buscador-eventos/BoletinEpidemiologico/2023_Boletín_epidemiologico_semana_14.pdf (accessed on 20 December 2023).
- Institudo National de Salud, Boletín Epidemiológico Semanal. Semana Epidemiológico 39. 2023. Available online: https://www.ins.gov.co/buscador-eventos/BoletinEpidemiologico/2023_Boletín_epidemiologico_semana_39.pdf (accessed on 20 December 2023).
- Vergara, H.D.; Gómez, C.H.; Faccini-Martinez, A.A.; Herrera, A.C.; López, M.J.; Camacho, C.; Muñoz, L.; Cruz-Saavedra, L.; Hernández, C.; Ramirez, J.D. Acute Chagas Disease Outbreak among Military Personnel, Colombia, 2021. Emerg. Infect. Dis. 2023, 29, 9. [Google Scholar] [CrossRef]
- Bastos, C.J.; Aras, R.; Mota, G.; Reis, F.; Dias, J.P.; de Jesus, R.S.; Freire, M.S.; de Araújo, E.G.; Prazeres, J.; Grassi, M.F. Clinical outcomes of thirteen patients with acute chagas disease acquired through oral transmission from two urban outbreaks in northeastern Brazil. PLoS Negl. Trop. Dis. 2010, 4, e711. [Google Scholar] [CrossRef]
- Marques, J.; Mendoza, I.; Noya, B.; Acquatella, H.; Palacios, I.; Marques-Mejias, M. ECG manifestations of the biggest outbreak of Chagas disease due to oral infection in Latin-America. Arq. Bras Cardiol. 2013, 101, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Parada, H.; Carrasco, H.A.; Añez, N.; Fuenmayor, C.; Inglessis, I. Cardiac involvement is a constant finding in acute Chagas’ disease: A clinical, parasitological and histopathological study. Int. J. Cardiol. 1997, 60, 49–54. [Google Scholar] [CrossRef]
- Jansen, A.M.; Xavier, S.C.D.C.; Roque, A.L.R. Trypanosoma cruzi transmission in the wild and its most important reservoir hosts in Brazil. Parasite Vectors 2018, 11, 502. [Google Scholar] [CrossRef] [PubMed]
- Cencig, S.; Coltel, N.; Truyens, C.; Carlier, Y. Parasitic loads in tissues of mice infected with Trypanosoma cruzi and treated with AmBisome. PLoS Negl. Trop. Dis. 2011, 5, e1216. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, A.R.; Hecht, M.M.; Guimaro, M.C.; Sousa, A.O.; Nitz, N. Pathogenesis of chagas’ disease: Parasite persistence and autoimmunity. Clin. Microbiol. Rev. 2011, 24, 592–630. [Google Scholar] [CrossRef]
- Magalhães-Santos, I.F.; Andrade, S.G. Participation of cytokines in the necrotic-inflammatory lesions in the heart and skeletal muscles of Calomys callosus infected with Trypanosoma cruzi. Mem. Inst. Oswaldo Cruz 2005, 100, 555–561. [Google Scholar] [CrossRef]
- Camandaroba, E.; Thé, T.S.; Pessina, D.H.; Andrade, S.G. Trypanosoma cruzi: Clones isolated from the Colombian strain, reproduce the parental strain characteristics, with ubiquitous histotropism. Int. J. Exp. Pathol. 2006, 87, 209–217. [Google Scholar] [CrossRef]
- Bowman, N.M.; Balasubramanian, S.; Gilman, R.H.; Parobek, C.; Calderon, M.; Waltmann, A.; Messenger, L.A.; Sanchez, L.; Bern, C.; Juliano, J.J. Working Group on Chagas Disease in Bolivia and Peru. Deep Sequencing to Detect Diversity of Trypanosoma cruzi Infection in Patients Coinfected with Human Immunodeficiency Virus and Chagas Disease. J. Infect. Dis. 2022, 225, 243–247. [Google Scholar] [CrossRef]
- Meza, S.K.; Kaneshima, E.N.; de Silva, O.; Gabriel, M.; de Araújo, S.M.; Gomes, M.L.; Monteiro, W.M.; Barbosa, M.D.; Toledo, M.J. Comparative pathogenicity in Swiss mice of Trypanosoma cruzi IV from northern Brazil and Trypanosoma cruzi II from southern Brazil. Exp. Parasitol. 2014, 146, 34–42. [Google Scholar] [CrossRef]
- Teston, A.P.M.; de Abreu, A.P.; Gruendling, A.P.; Bahia, M.T.; Gomes, M.L.; de Araújo, S.M.; Ornelas Toledo, M.J. Differential parasitological, molecular, and serological detection of Trypanosoma cruzi I, II, and IV in blood of experimentally infected mice. Exp. Parasitol. 2016, 166, 44–50. [Google Scholar] [CrossRef]
- Moncayo, A.; Silveira, A.C. Current trends and future prospects for control of Chagas disease. In American Trypanosomiasis Chagas Disease: One Hundred Years of Research; Telleria, J., Tibayrenc, M., Eds.; Elsevier: Amsterdam, The Netherlands, 2010; pp. 55–82. [Google Scholar]
- Figueiredo, V.P.; Junior, E.S.L.; Lopes, L.R.; Simões, N.F.; Penitente, A.R.; Bearzoti, E.; Vieira, P.M.A.; Schulz, R.; Talvani, A. High fat diet modulates inflammatory parameters in the heart and liver during acute Trypanosoma cruzi infection. Int. Immunopharmacol. 2018, 64, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Dhanyalayam, D.; Thangavel, H.; Lizardo, K.; Oswal, N.; Dolgov, E.; Perlin, D.S.; Nagajyothi, J.F. Sex Differences in Cardiac Pathology of SARS-CoV-2 Infected and Trypanosoma cruzi Co-infected Mice. Front. Cardiovasc. Med. 2022, 9, 783974. [Google Scholar] [CrossRef] [PubMed]
- Nolan, M.S.; Hochberg, N.S. Chagas Disease in HIV-Infected Patients: It’s Time to Consider the Diagnosis. Am. J. Trop. Med. Hyg. 2021, 105, 545–546. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, G.; Salazar-Alcalá, E.; Hernández, F.; Deglesne, P.A.; Bello, Z.D.; de Noya, B.A.; Noya, O.; Fernández-Mestre, M. Polymorphisms of the TLR4 gene: Risk factor for chronicity and severity in oral vectorial Chagas disease. Exp. Parasitol. 2022, 238, 108243. [Google Scholar] [CrossRef] [PubMed]
- Wesley, M.; Moraes, A.; Rosa, A.C.; Lott Carvalho, J.; Shiroma, T.; Vital, T.; Dias, N.; de Carvalho, B.; do Amaral Rabello, D.; Borges, T.K.D.S.; et al. Correlation of Parasite Burden, kDNA Integration, Autoreactive Antibodies, and Cytokine Pattern in the Pathophysiology of Chagas Disease. Front. Microbiol. 2019, 10, 1856. [Google Scholar] [CrossRef] [PubMed]
- Rassi, A., Jr.; Marin, J.A. Chronic Chagas cardiomyopathy: A review of the main pathogenic mechanisms and the efficacy of aetiological treatment following the BENznidazole Evaluation for Interrupting Trypanosomiasis (BENEFIT) trial. Mem. Inst. Oswaldo Cruz 2017, 112, 224–235. [Google Scholar] [CrossRef]
- Antunes, D.; Marins-Dos-Santos, A.; Ramos, M.T.; Mascarenhas, B.A.S.; Moreira, C.J.C.; Farias-de-Oliveira, D.A.; Savino, W.; Monteiro, R.Q.; de Meis, J. Oral Route Driven Acute Trypanosoma cruzi Infection Unravels an IL-6 Dependent Hemostatic Derangement. Front. Immunol. 2019, 10, 1073. [Google Scholar] [CrossRef]
- Magalhães, L.M.D.; Gollob, K.J.; Zingales, B.; Dutra, W.O. Pathogen diversity, immunity, and the fate of infections: Lessons learned from Trypanosoma cruzi human-host interactions. Lancet Microbe 2022, 3, e711–e722. [Google Scholar] [CrossRef]
- Marcon, G.E.; de Albuquerque, D.M.; Batista, A.M.; Andrade, P.D.; Almeida, E.A.; Guariento, M.E.; Teixeira, M.A.; Costa, S.C. Trypanosoma cruzi: Parasite persistence in tissues in chronic chagasic Brazilian patients. Mem. Inst. Oswaldo Cruz 2011, 106, 85–91. [Google Scholar] [CrossRef]
- Pereira, K.S.; Schmidt, F.L.; Barbosa, R.L.; Guaraldo, A.M.; Franco, R.M.; Dias, V.L.; Passos, L.A. Transmission of chagas disease (American trypanosomiasis) by food. Adv Food Nutr Res. 2010, 59, 63–85. [Google Scholar]
- Barros, F.D.N.L.; Júnior, F.D.S.; de Mamedes Costa, S.; de Farias, D.M.; Moura, M.A.O.; Júnior, P.S.B.; Scofield, A. First report of natural infection by Trypanosoma cruzi in secretions of the scent glands and myocardium of Philander opossum (Marsupialia: Didelphidae): Parasitological and clinicopathological findings. Vet. Parasitol. Reg. Stud. Rep. 2020, 22, 100463. [Google Scholar] [CrossRef] [PubMed]
- Suárez, D.C.; Rey, Á.P.; Orduz, M.L.; Prada, R.L.; Tarazona, Z. Supervivencia de Trypanosoma cruzi en bebidas experimentalmente contaminadas [Survival of Trypanosoma cruzi in experimentally contaminated drinks]. Biomedica 2012, 32, 134–138. [Google Scholar] [PubMed]
- Cardoso, A.V.; Lescano, S.A.; Amato Neto, V.; Gakiya, E.; Santos, S.V. Survival of Trypanosoma cruzi in sugar cane used to prepare juice. Rev. Inst. Med. Trop. São Paulo 2006, 48, 287–289. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, R.L.; Dias, V.L.; Pereira, K.S.; Schmidt, F.L.; Franco, R.M.; Guaraldo, A.M.; Alves, D.P.; Passos, L.A. Survival in vitro and virulence of Trypanosoma cruzi in açaí pulp in experimental acute Chagas disease. J. Food Prot. 2012, 75, 601–606. [Google Scholar] [CrossRef] [PubMed]
- Nolan, M.S.; Tonussi Mendes, J.E.; Perez Riera, A.R.; Laporta, G.Z. Oral Trypanosoma cruzi Transmission Resulting in Advanced Chagasic Cardiomyopathy in an 11-Month-Old Male. Case Rep. Infect. Dis. 2020, 2020, 8828950. [Google Scholar] [CrossRef] [PubMed]
- Tyler, K.M.; Engman, D.M. The life cycle of Trypanosoma cruzi revisited. Int. J. Parasitol. 2001, 31, 472–481. [Google Scholar] [CrossRef] [PubMed]
- Sangenis, L.H.C.; Nielebock, M.A.P.; Santos, C.D.S.; Silva, M.C.C.D.; Bento, G.M.R. Chagas disease transmission by consumption of game meat: Systematic review. Rev. Bras. Epidemiol. 2016, 19, 803–811. [Google Scholar] [CrossRef]
- Sangenis, L.H.C.; Saraiva, R.M.; Georg, I.; De Castro, L.; dos Santos Lima, V.; Roque, A.L.R.; Bóia, M.N. Autochthonous transmission of Chagas disease in Rio de Janeiro State, Brazil: A clinical and eco-epidemiological study. BMC Infect. Dis. 2015, 15, 1–12. [Google Scholar] [CrossRef]
- Colorado, J.W.P.; Botero, Á.B.; Rodríguez, C.A.S. Percepción y uso de mamíferos silvestres por comunidades campesinas andinas de Génova, Quindío, Colombia. Boletín Científico. Cent. Mus. 2014, 18, 78–93. [Google Scholar]
- Cardona-Castro, N.; Beltrán, J.C.; Ortiz-Bernal, A.; Vissa, V. Detection of Mycobacterium leprae DNA in nine-banded armadillos (Dasypus novemcinctus) from the Andean region of Colombia. Lepr. Rev. 2009, 80, 424–431. [Google Scholar] [CrossRef]
- Gómez, J.; Van Vliet, N.; Restrepo, S.; Daza, E.; Moreno, J.; Cruz-Antia, D.; Nasi, R. Use and trade of bushmeat in Colombia Relevance to rural livelihoods. Cent. Int. For. Res. (CIFOR) Infobriefs 2016, 159. [Google Scholar] [CrossRef]
- Rodríguez-Monguí, E.; Cantillo-Barraza, O.; Prieto-Alvarado, F.E.; Cucunubá, Z.M. Heterogeneity of Trypanosoma cruzi infection rates in vectors and animal reservoirs in Colombia: A systematic review and meta-analysis. Parasite Vectors 2019, 12, 308. [Google Scholar] [CrossRef] [PubMed]
- Rocha, F.L.; Roque, A.L.; de Lima, J.S.; Cheida, C.C.; Lemos, F.G.; de Azevedo, F.C.; Arrais, R.C.; Bilac, D.; Herrera, H.M.; Mourão, G.; et al. Trypanosoma cruzi infection in neotropical wild carnivores (Mammalia: Carnivora): At the top of the T. cruzi transmission chain. PLoS ONE 2013, 8, e67463. [Google Scholar] [CrossRef] [PubMed]
- Marinkelle, C.J. The prevalence of Trypanosoma (Schizotrypanum) cruzi cruzi infection in Colombian monkeys and marmosets. Ann. Trop. Med. Parasitol. 1982, 76, 121–124. [Google Scholar] [CrossRef] [PubMed]
- Enríquez Vázquez, P.; Mariaca Méndez, R.; Retana Guiascón, O.G. Uso medicinal de la fauna silvestre en los Altos de Chiapas, México. Interciencia 2006, 31, 491–499. [Google Scholar]
- Asociación Colombiana de Parasitología. Simposios XVII Congreso Colombiano de Parasitología y Medicina Tropical. Biomédica 2015, 35 (Suppl. S4), 17–71. [Google Scholar]
- de Noya, B.A.; Colmenares, C.; Guevara, R.R.; Bello, Z.D.; Noya, O.N.O. La transmisión oral en la enfermedad de Chagas. Rev. Fac. Med. 2010, 33, 78–86. [Google Scholar]
- Toso, A.; Vial, F.; Galanti, N. Transmisión de la enfermedad de Chagas por vía oral. Ver. Med. Chile. 2011, 139, 258–266. [Google Scholar] [CrossRef]
- Orozco Rodríguez, J.R.; Agencia AUPEC Ciencia al Día. Los Campesinos Han Comprobado Que Beber su Sangre Combate el Asma. Ciencia al Día. Available online: https://aupec.univalle.edu.co/informes/diciembre97/boletin57/sietecarnes.html (accessed on 20 December 2023).
- Barreto, M.; Pablo, B.; D’Alessandro, A. Colombian armadillos: Stomach contents and infection with Trypanosoma cruzi. J. Mammal. 1985, 66, 188–193. [Google Scholar] [CrossRef]
- Balamayooran, G.; Pena, M.; Sharma, R.; Truman, R.W. The armadillo as an animal model and reservoir host for Mycobacterium leprae. Clin. Dermatol. 2015, 33, 108–115. [Google Scholar] [CrossRef]
- Chacón, F.; Muñoz-San Martín, C.; Bacigalupo, A.; Álvarez-Duhart, B.; Solís, R.; Cattan, P.E. Trypanosoma cruzi Parasite Load Modulates the Circadian Activity Pattern of Triatoma infestans. Insects 2022, 13, 76. [Google Scholar] [CrossRef] [PubMed]
- Valença-Barbosa, C.; Finamore-Araujo, P.; Moreira, O.C.; Vergara-Meza, J.G.; Alvarez, M.V.N.; Nascimento, J.R.; Almeida, C.E. Genotypic Trypanosoma cruzi distribution and parasite load differ ecotypically and according to parasite genotypes in Triatoma brasiliensis from endemic and outbreak areas in Northeastern Brazil. Acta Trop. 2021, 222, 106054. [Google Scholar] [CrossRef] [PubMed]
- Moreira, O.C.; Verly, T.; Finamore-Araujo, P.; Gomes, S.A.O.; Lopes, C.M.; de Sousa, D.M.; Azevedo, L.R.; da Mota, F.F.; d’Avila-Levy, C.M.; Santos-Mallet, J.R.; et al. Development of conventional and real-time multiplex PCR-based assays for estimation of natural infection rates and Trypanosoma cruzi load in triatomine vectors. Parasite Vectors 2017, 10, 404. [Google Scholar] [CrossRef] [PubMed]
- Mazza, S.; Montana, A.; Benitez, C.; Janzi, E.Z. Transmisión de Schizotrypanum cruzi al niño por leche de la madre con enfermedad de Chagas. Mepra 1936, 28, 41–46. [Google Scholar]
- Norman, F.F.; López-Vélez, R. Chagas disease and breast-feeding. Emerg. Infect. Dis. 2013, 19, 1561–1566. [Google Scholar] [CrossRef]
- Bittencourt, A.L.; Sadigursky, M.; Silva, A.A.D.; Menezes, C.A.; Marianetti, M.M.; Guerra, S.C.; Sherlock, Í. Evaluation of Chagas’ disease transmission through breast-feeding. Mem. Inst. Oswaldo Cruz 1988, 83, 37–39. [Google Scholar] [CrossRef]
- Medina-Lopes, M.D.D.; Macêdo, V. Trypanosoma cruzi no colostro humano. Rev. Soc. Bras. Med. Trop. 1983, 16, 170. [Google Scholar] [CrossRef]
- Ferreira, C.S.; Martinho, P.C.; Amato Neto, V.; Cruz, R.R.B. Pasteurization of human milk to prevent transmission of Chagas disease. Rev. Inst. Med. Trop. Sao Paulo 2001, 43, 161–162. [Google Scholar] [CrossRef]
- Dias, J.P.; Bastos, C.; Araújo, E.; Mascarenhas, A.V.; Martins Netto, E.; Grassi, F.; Aras, R. Acute Chagas disease outbreak associated with oral transmission. Rev. Soc. Bras. Med. Trop. 2008, 41, 296–300. [Google Scholar] [CrossRef]
- Calvo-Méndez, M.L.; Nogueda-Torres, B.; Alejandre-Aguilar, R.; Cortés-Jiménez, M. Experimental Trypanosoma cruzi infection via contaminated water and food. Rev. Latinoam. Microbiol. 1994, 36, 67–69. [Google Scholar]
- Klotz, S.A.; Shirazi, F.M.; Boesen, K.; Beatty, N.L.; Dorn, P.L.; Smith, S.; Schmidt, J.O. Kissing Bug (Triatoma spp.) Intrusion into Homes: Troublesome Bites and Domiciliation. Environ. Health Insights 2016, 10, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Beatty, N.L.; Behrens-Bradley, N.; Love, M.; McCants, F.; Smith, S.; Schmidt, J.O.; Hamer, S.A.; Dorn, P.L.; Ahmad, N.; Klotz, S.A. Rapid detection of human blood in triatomines (kissing bugs) utilizing a lateral flow immunochromatographic assay—A pilot study. Mem. Inst. Oswaldo Cruz 2019, 114, e190047. [Google Scholar] [CrossRef] [PubMed]
- Curtis-Robles, R.; Wozniak, E.J.; Auckland, L.D.; Hamer, G.L.; Hamer, S.A. Combining Public Health Education and Disease Ecology Research: Using Citizen Science to Assess Chagas Disease Entomological Risk in Texas. PLoS Negl. Trop. Dis. 2015, 9, e0004235. [Google Scholar] [CrossRef]
- Velásquez-Ortiz, N.; Hernández, C.; Cantillo-Barraza, O.; Ballesteros, N.; Cruz-Saavedra, L.; Herrera, G.; Buitrago, L.S.; Soto, H.; Medina, M.; Palacio, J.; et al. Trypanosoma cruzi Parasite Burdens of Several Triatomine Species in Colombia. Trop. Med. Infect. Dis. 2022, 7, 445. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, E.; Ballesteros, V.L.; Llanos, I.V. Chagas Agudo en San Juan de Urabá_Antioquia, 2023: Desde la clínica al diagnóstico y su intervención. Actu Biol. 2023, 45 (Suppl. S1), 47–54. [Google Scholar]
- Pérez-Doria, A.; Zabala-Monterroza, W.; Bedoya-Polo, A.; Bejarano, E. Aislamiento de Trypanosoma cruzi I em población escolar afectada por enfermedad de Chagas en el municipio El Roble, Sucre. Actu Biol. 2023, 45 (Suppl. S1), 47–54. [Google Scholar]
- Cantillo-Barraza, O.; Chaverra, D.; Marcet, P.; Arboleda-Sánchez, S.; Triana-Chávez, O. Trypanosoma cruzi transmission in a Colombian Caribbean region suggests that secondary vectors play an important epidemiological role. Parasite Vectors 2014, 7, 381. [Google Scholar] [CrossRef]
- Lent, H.; Wygodzinsky, P.W. Revision of the Triatominae (Hemiptera, Re-duviidae), and their significance as vectors of Chagas’ disease. Bull. Am. Mus. Nat. Hist. 1979, 163, 123–520. [Google Scholar]
- Mesa, P.; Cantillo, O.; Quintero, J.C. Evaluación de la observancia y la cobertura de la vigilancia entomológica de la enfermedad de Chagas en la Mesa, Cundinamarca. Biomédica 2022, 42 (Suppl. 3), 113–254. Available online: https://revistabiomedica.org/index.php/biomedica/article/download/6798/5177/38625 (accessed on 20 December 2023).
- Beatty, N.L.; Bhosale, C.R.; Torhorst, C.W.; Burkett-Cadena, N.D.; Oi, F.M.; Forsyth, C.J.; Wisely, S.M. Integrated pest management strategies targeting the Florida kissing bug, Triatoma sanguisuga: Preventing this vector of Chagas disease from invading your home. Curr. Res. Parasitol. Vector Borne Dis. 2023, 4, 100144. [Google Scholar] [CrossRef]
- Roque, A.L.; Xavier, S.C.; da Rocha, M.G.; Duarte, A.C.; D’Andrea, P.S.; Jansen, A.M. Trypanosoma cruzi transmission cycle among wild and domestic mammals in three areas of orally transmitted Chagas disease outbreaks. Am. J. Trop. Med. Hyg. 2008, 79, 742–749. [Google Scholar] [CrossRef] [PubMed]
- Xavier, S.C.; Roque, A.L.; Lima, V.d.S.; Monteiro, K.J.; Otaviano, J.C.; Ferreira da Silva, L.F.; Jansen, A.M. Lower richness of small wild mammal species and chagas disease risk. PLoS Negl. Trop. Dis. 2012, 6, e1647. [Google Scholar] [CrossRef] [PubMed]
- Deane, M.P.; Lenzi, H.L.; Jansen, A. Trypanosoma cruzi: Vertebrate and invertebrate cycles in the same mammal host, the opossum Didelphis marsupialis. Mem. Inst. Oswaldo Cruz 1984, 79, 513–515. [Google Scholar] [CrossRef] [PubMed]
- Urdaneta-Morales, S.; Nironi, I. Trypanosoma cruzi in the anal glands of urban opossums. I--Isolation and experimental infections. Mem. Inst. Oswaldo Cruz 1996, 91, 399–403. [Google Scholar] [CrossRef]
- Carreira, J.C.; Jansen, A.M.; de Nazareth Meirelles, M.; Costa e Silva, F.; Lenzi, H.L. Trypanosoma cruzi in the scent glands of Didelphis marsupialis: The kinetics of colonization. Exp. Parasitol. 2001, 97, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Torhorst, C.W.; White, Z.S.; Bhosale, C.R.; Beatty, N.L.; Wisely, S.M. Identification of the parasite, Trypanosoma cruzi, in multiple tissues of epidemiological significance in the Virginia opossum (Didelphis virginiana): Implications for environmental and vertical transmission routes. PLoS Negl. Trop. Dis. 2022, 16, e0010974. [Google Scholar] [CrossRef]
- Cantillo-Barraza, O.; Garcés, E.; Gómez-Palacio, A.; Cortés, L.A.; Pereira, A.; Marcet, P.L.; Jansen, A.M.; Triana-Chávez, O. Eco-epidemiological study of an endemic Chagas disease region in northern Colombia reveals the importance of Triatoma maculata (Hemiptera: Reduviidae), dogs and Didelphis marsupialis in Trypanosoma cruzi maintenance. Parasite Vectors 2015, 8, 1–10. [Google Scholar] [CrossRef]
- Cruz-Saavedra, L.; Jaimes, J.; Cantillo, O.; Hernández, C.; Medina, M.; Leal, B.; Martínez, L.; Valdivieso, S.; Medina, M.; Hidalgo, A.R.; et al. Uso de herramientas NGS en la caracterización y el entendimiento de la transmisión de la enfermedad de Chagas por vía oral en Colombia. Biomédica 2022, 42 (Suppl. 3), 31–112. Available online: https://revistabiomedica.org/index.php/biomedica/article/download/6797/5176/38624 (accessed on 20 December 2023).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
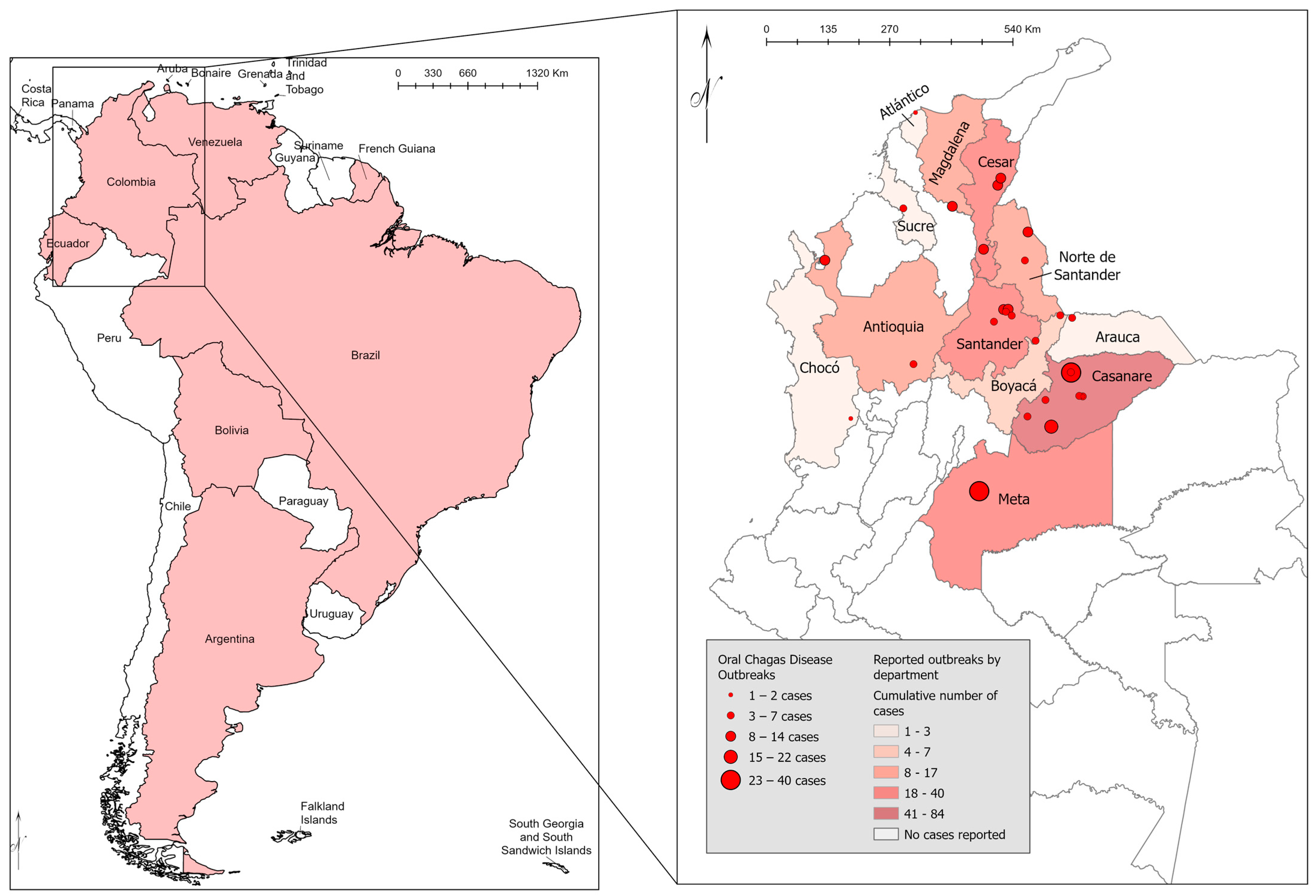
| City/Department | Suspected or Confirmed Oral Source of T. cruzi | Number of Cases | Year | Reference |
|---|---|---|---|---|
| Tibú, Norte de Santander | Unknown | 14 | 1992 | Bohorquez, et al., 1992 [19] |
| Guamal, Magdalena | Palm wine | 13 | 1999 | Cáceres, et al., 1999 [20] |
| Lebrija, Santander | Orange juice | 10 | 2008 | Hernández, et al., 2009 [21] |
| Girón, Santander | Unknown | 5 | 2008–2009 | Zambrano, et al., 2010 [22] |
| Piedecuesta, Santander | Unknown | 5 | 2008–2009 | Zambrano, et al., 2010 [22] |
| Bucaramanga | Orange and/or tangerine juice | 9 | 2009 | Rameríz, et al., 2013 [23] |
| San Vicente de Chucuri, Santander | Triatomine fecal-contaminated food | 3 | 2010 | Rueda, et al., 2014 [24] |
| Aguachica, Cesar | Unknown | 12 | 2010 | Soto, et al., 2014 [25] |
| Turbo, Antioquia | D. marsupialis fecal and/or anal secretion contaminated food | 11 | 2010 | Ríos, et al., 2011 [26] |
| Paz de Ariporo, Casanare | Food/beverages contaminated by triatomine feces or D. marsupialis fecal and/or anal secretion | 40 | 2014 | Zuleta-Dueñas, et al., 2017 [27] |
| Trinidad, Casanare | Contaminated food | 6 | 2015 | Prensa Libre Casanare, 2015 [28] |
| San Luis de Palenque, Casanare | Contaminated food | 4 | 2016 | Instituto Nacional de Salud, BES, Número 18, 2017 [29] |
| Paz de Ariporo, Casanare | Contaminated food | 4 | 2017 | Prensa Libre Casanare, 2017 [30] |
| Puerto Colombia, Atlántico | Contaminated food | Family; 2 deaths | 2019 | Instituto Nacional de Salud, BES, Semena 33, 2019 [31] |
| Los Roble, Cesar | Contaminated food | 3 | 2019 | Instituto Nacional de Salud, BES, Semena 33, 2019 [31] |
| Maní, Casanare | Contaminated food and/or beverages | 22 | 2019 | Instituto Nacional de Salud, BES, Semena 33, 2019 [31] |
| San Luis, Antioquia | Contaminated food | 4 | 2019 | Instituto Nacional de Salud, BES, Semena 33, 2019 [31] |
| San José del Palmar, Chocó | Armadillo blood | 2 | 2019 | Instituto Nacional de Salud, BES, Semena 33, 2019 [31] |
| Yopal, Casanare | Contaminated food | 4 | 2020 | Prensa Libre Casanare, 2020 [32] |
| La Jagua de Ibirico, Cesar | Contaminated food | 11 | 2021 | Instituto Nacional de Salud, BES, Semana 20, 2021 [33] |
| Trinidad, Casanare | Contaminated food | 1 | 2021 | Instituto Nacional de Salud, BES, Semana 6, 2021 [34] |
| Cubara, Boyacá | D. marsupialis fecal and/or anal secretion contaminated food | 5 | 2021 | Gutiérrez, S. A., et al., 2023 [35] |
| Sardinata, Norte de Santander | Contaminated food | 3 | 2022 | Instituto Nacional de Salud, BES, Semana 11, 2022 [36] |
| Arauquita, Arauca | Contaminated food | 3 | 2022 | Instituto Nacional de Salud, BES, Semana 18, 2022 [37] |
| Maracavita, Santander | Contaminated food | 3 | 2022 | Instituto Nacional de Salud, BES, Semana 18, 2022 [37] |
| Becerril, Cesar | Contaminated food | 11 | 2022 | Instituto Nacional de Salud, BES, Semana 18, 2022 [37] |
| Tauramena, Casanare | Contaminated food | 1 | 2023 | Instituto Nacional de Salud, BES, Semana 14, 2023 [38] |
| Granada, Meta | Contaminated food | 40 | 2023 | Instituto Nacional de Salud, BES, Semana 39, 2023 [39] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beatty, N.L.; Arango-Ferreira, C.; Gual-Gonzalez, L.; Zuluaga, S.; Nolan, M.S.; Cantillo-Barraza, O. Oral Chagas Disease in Colombia—Confirmed and Suspected Routes of Transmission. Trop. Med. Infect. Dis. 2024, 9, 14. https://doi.org/10.3390/tropicalmed9010014
Beatty NL, Arango-Ferreira C, Gual-Gonzalez L, Zuluaga S, Nolan MS, Cantillo-Barraza O. Oral Chagas Disease in Colombia—Confirmed and Suspected Routes of Transmission. Tropical Medicine and Infectious Disease. 2024; 9(1):14. https://doi.org/10.3390/tropicalmed9010014
Chicago/Turabian StyleBeatty, Norman L., Catalina Arango-Ferreira, Lídia Gual-Gonzalez, Sara Zuluaga, Melissa S. Nolan, and Omar Cantillo-Barraza. 2024. "Oral Chagas Disease in Colombia—Confirmed and Suspected Routes of Transmission" Tropical Medicine and Infectious Disease 9, no. 1: 14. https://doi.org/10.3390/tropicalmed9010014